Updated 10 April 2020
This page serves as an archive of previous MIT Emergency Ventilator prototypes. These designs have been retired. Please use the most up to date information on the Mechanical page.
Version 2 – Retired
CAD files for the Version 2 design and a pre-production model can be found on our Downloads page.
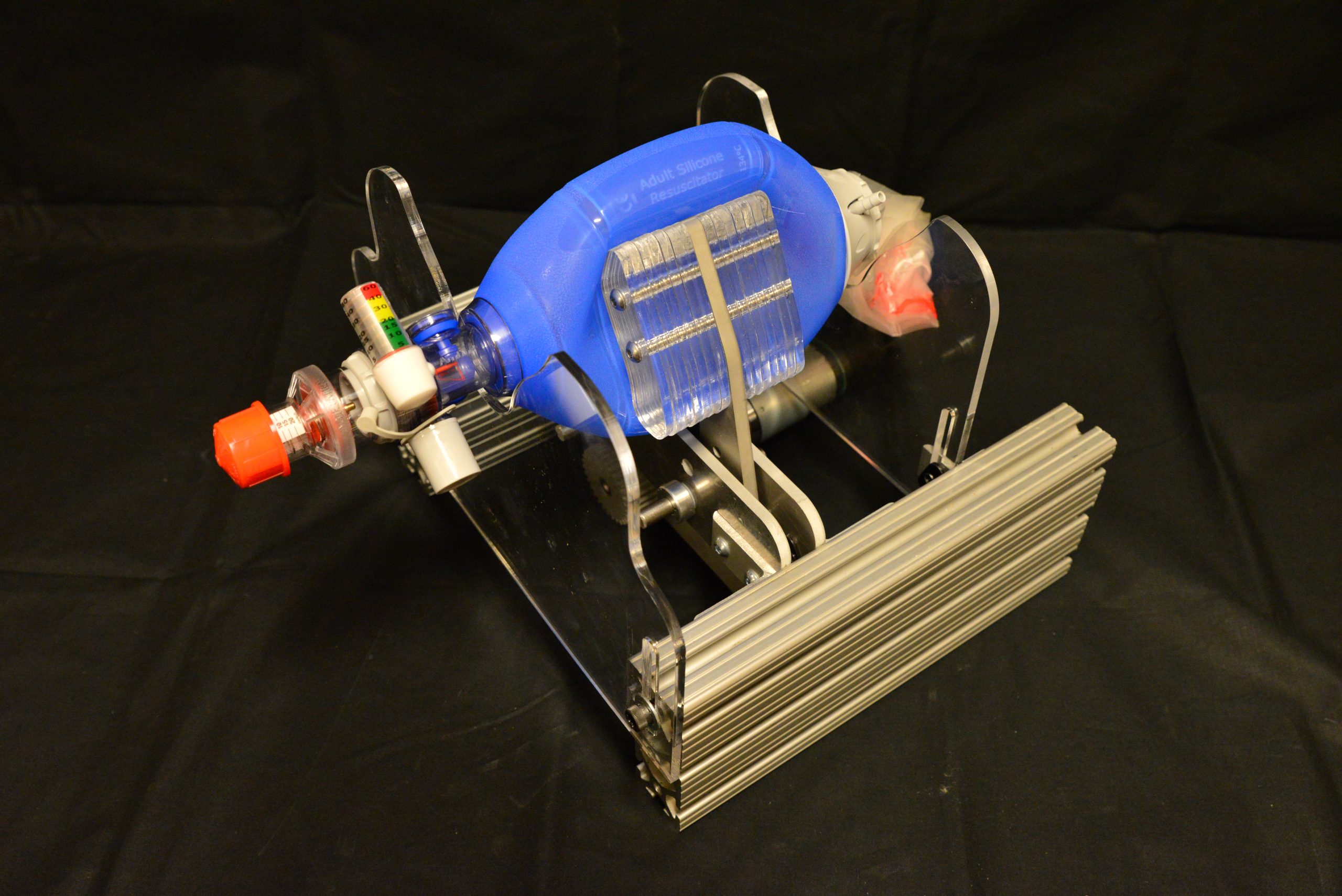
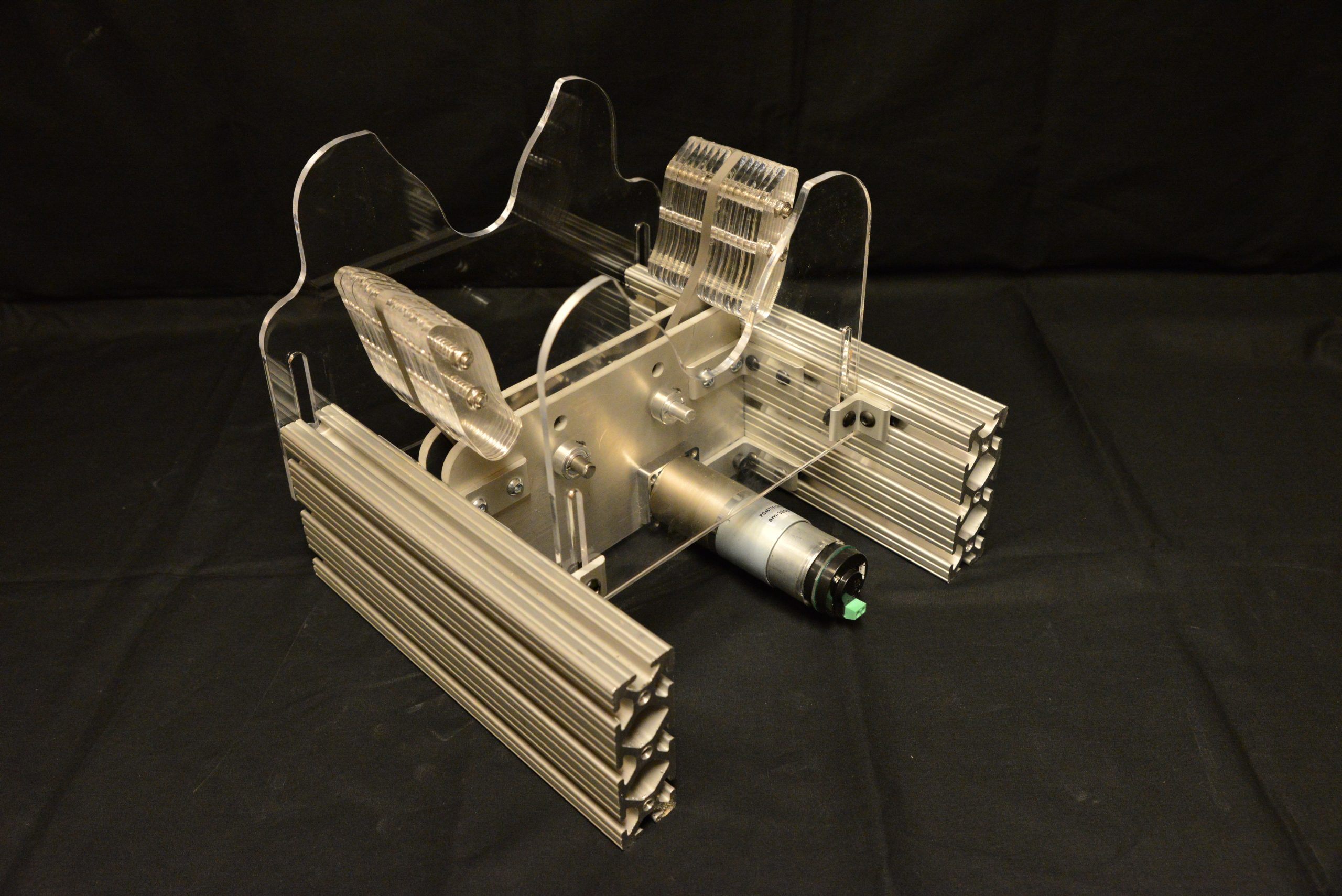

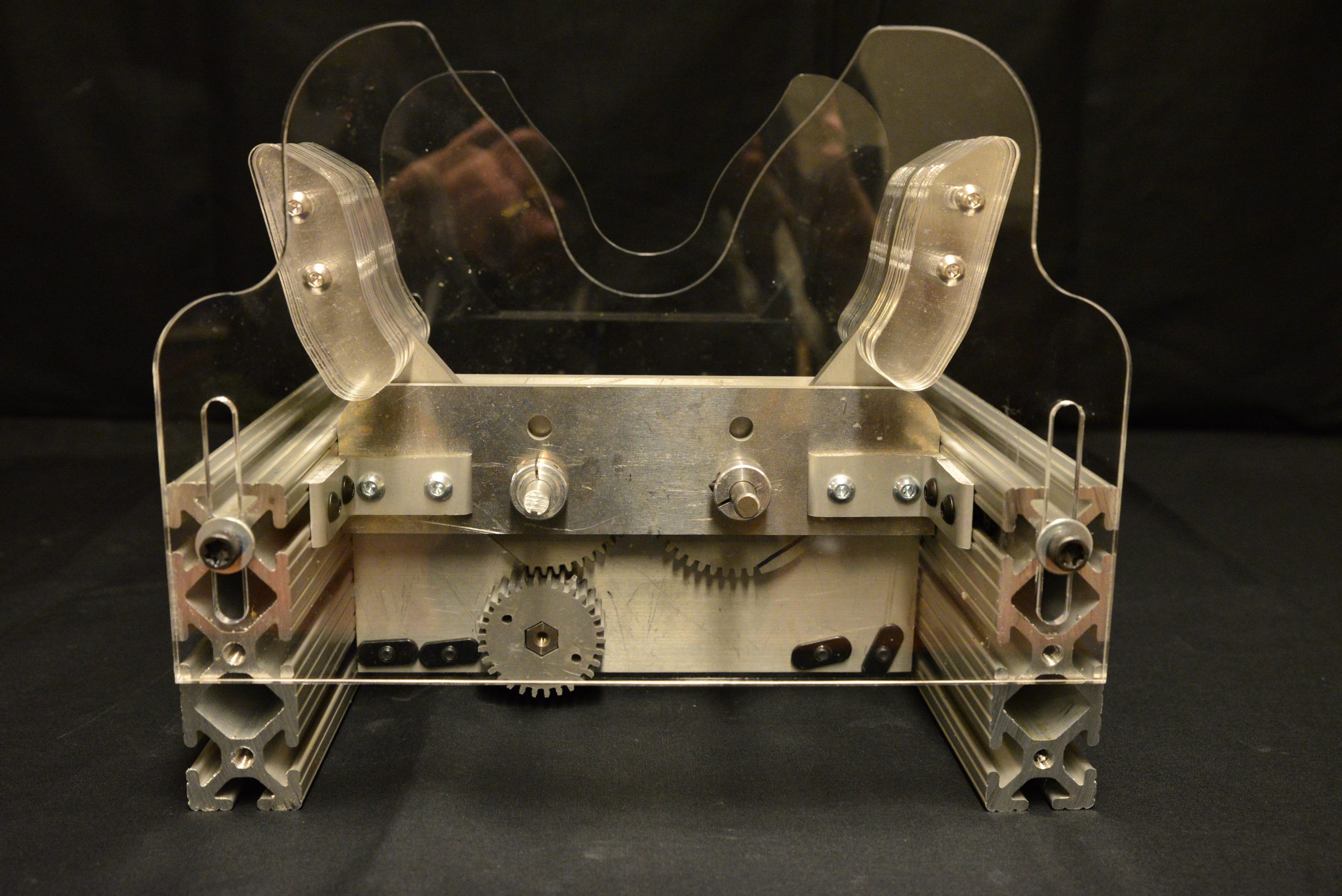
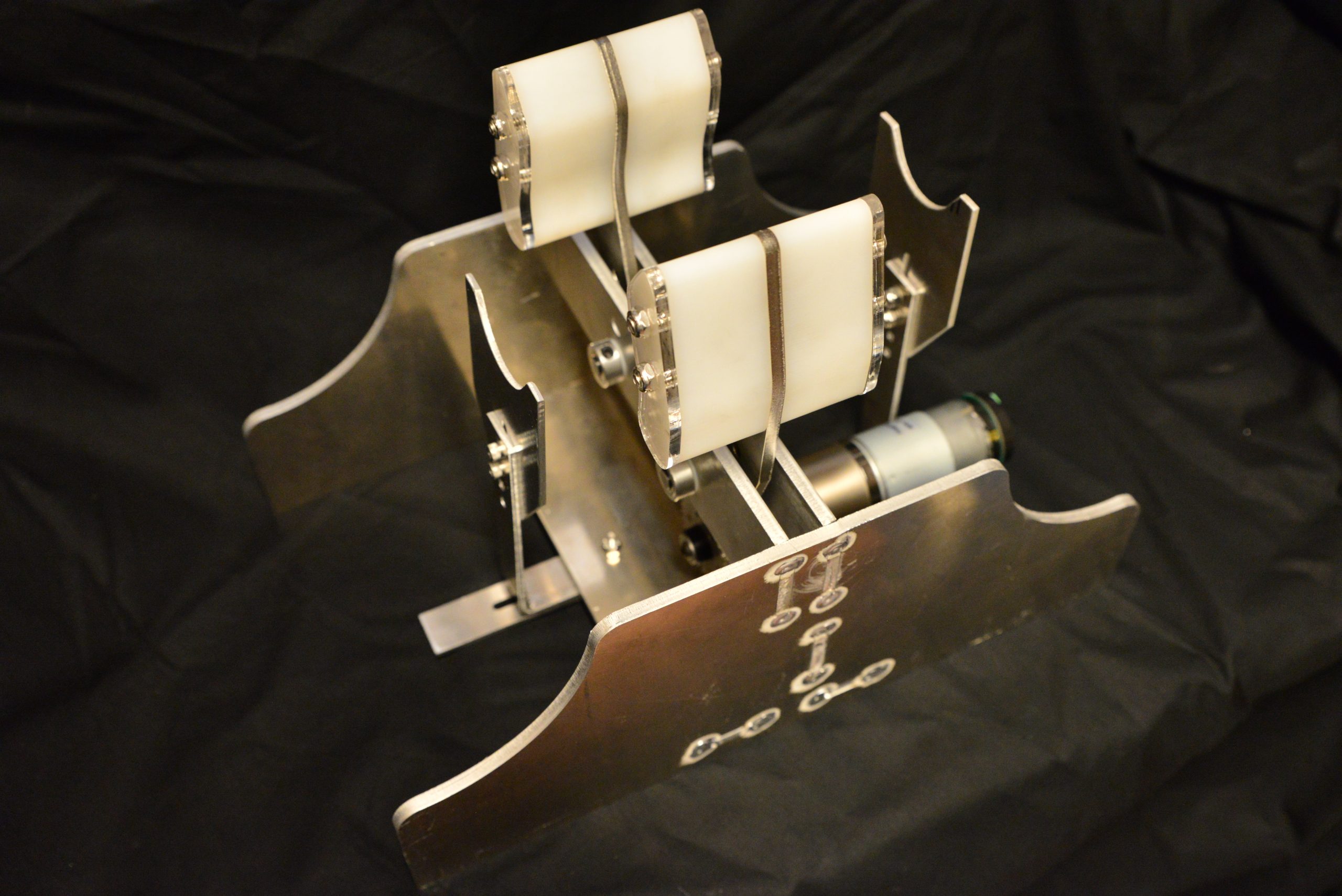
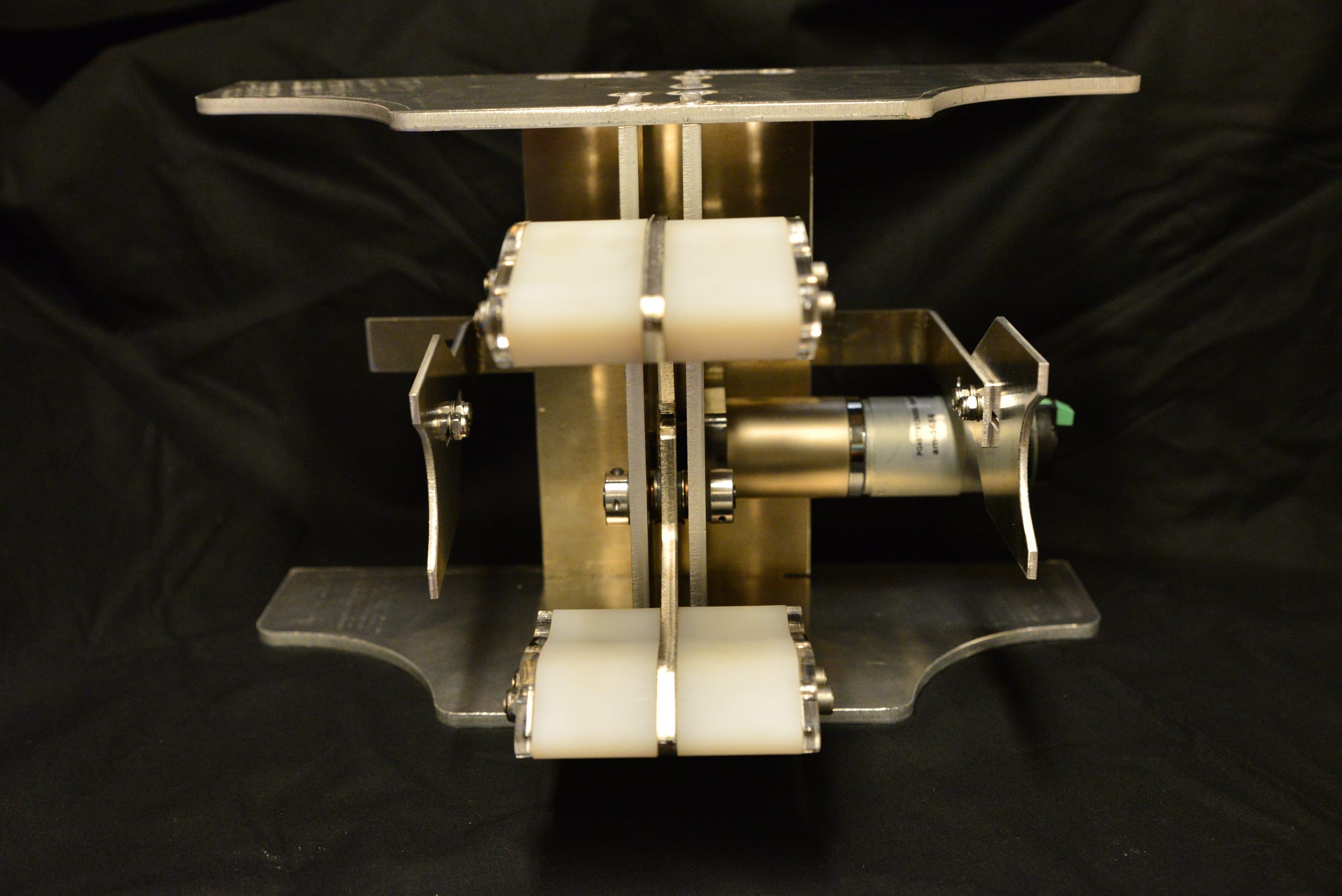
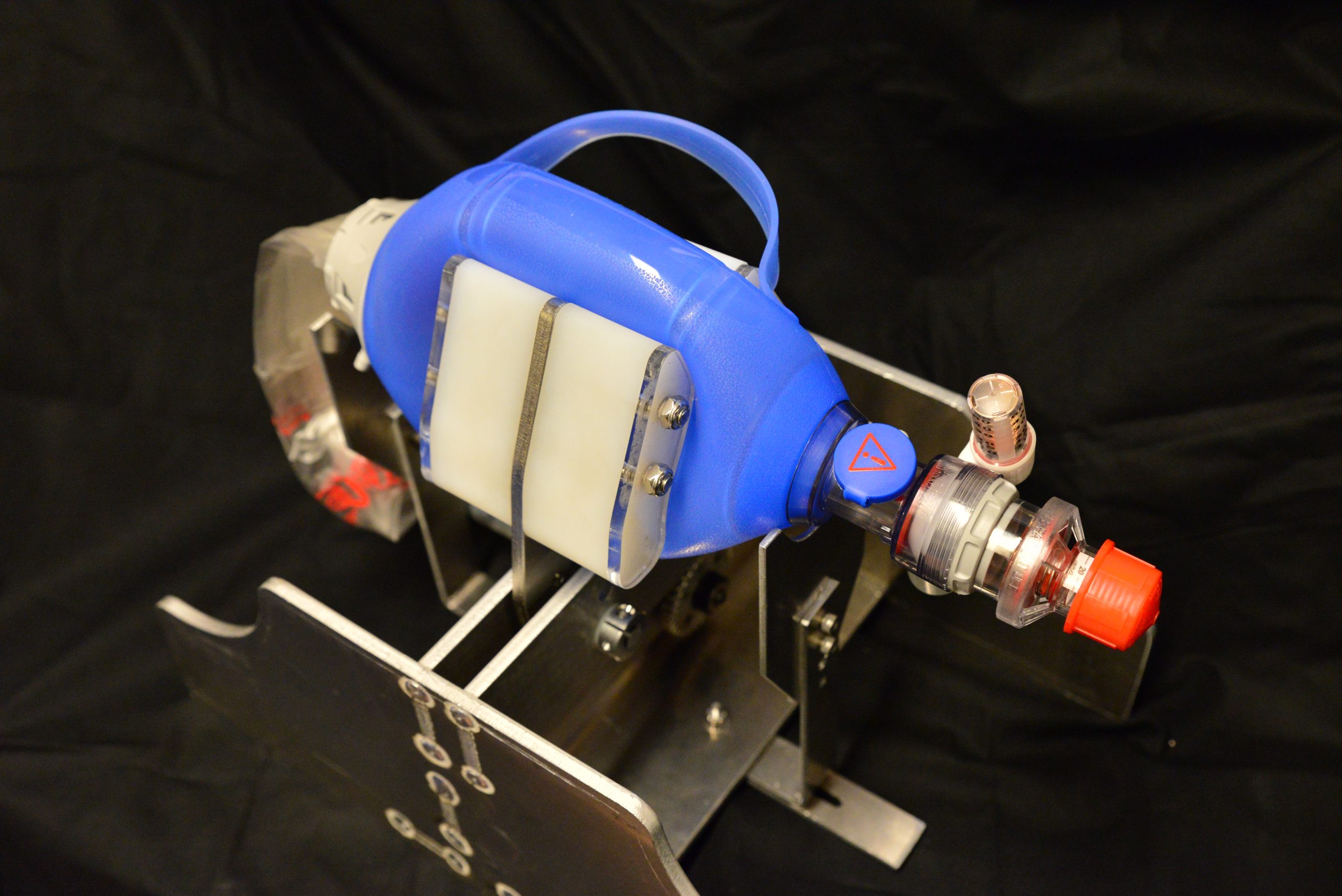
Notice that the bag support plates are adjustable both horizontally and vertically. This allows different bags to be supported between the arms. Additionally, the bag is entirely exposed from the top. This allows a clinician to immediately and intuitively grab and remove the bag from the device and squeeze manually, in case of machine failure. This safety feature is supported by a back-drivable gear train. This ensures that even if the device fails with the arms closed, a clinician can pull the arms apart by hand to remove the bag.
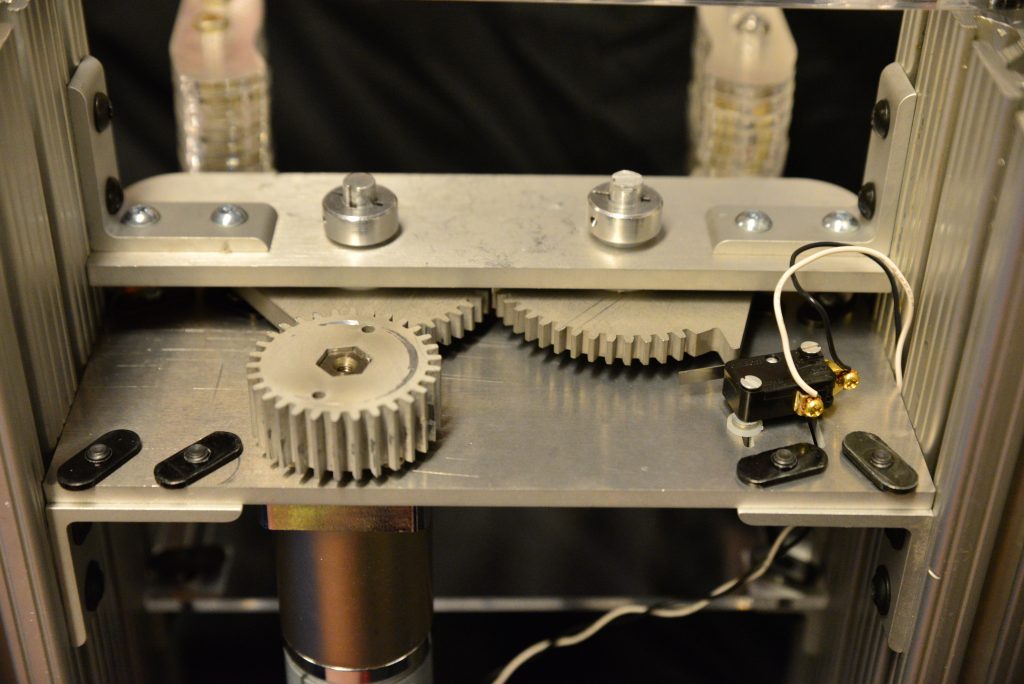
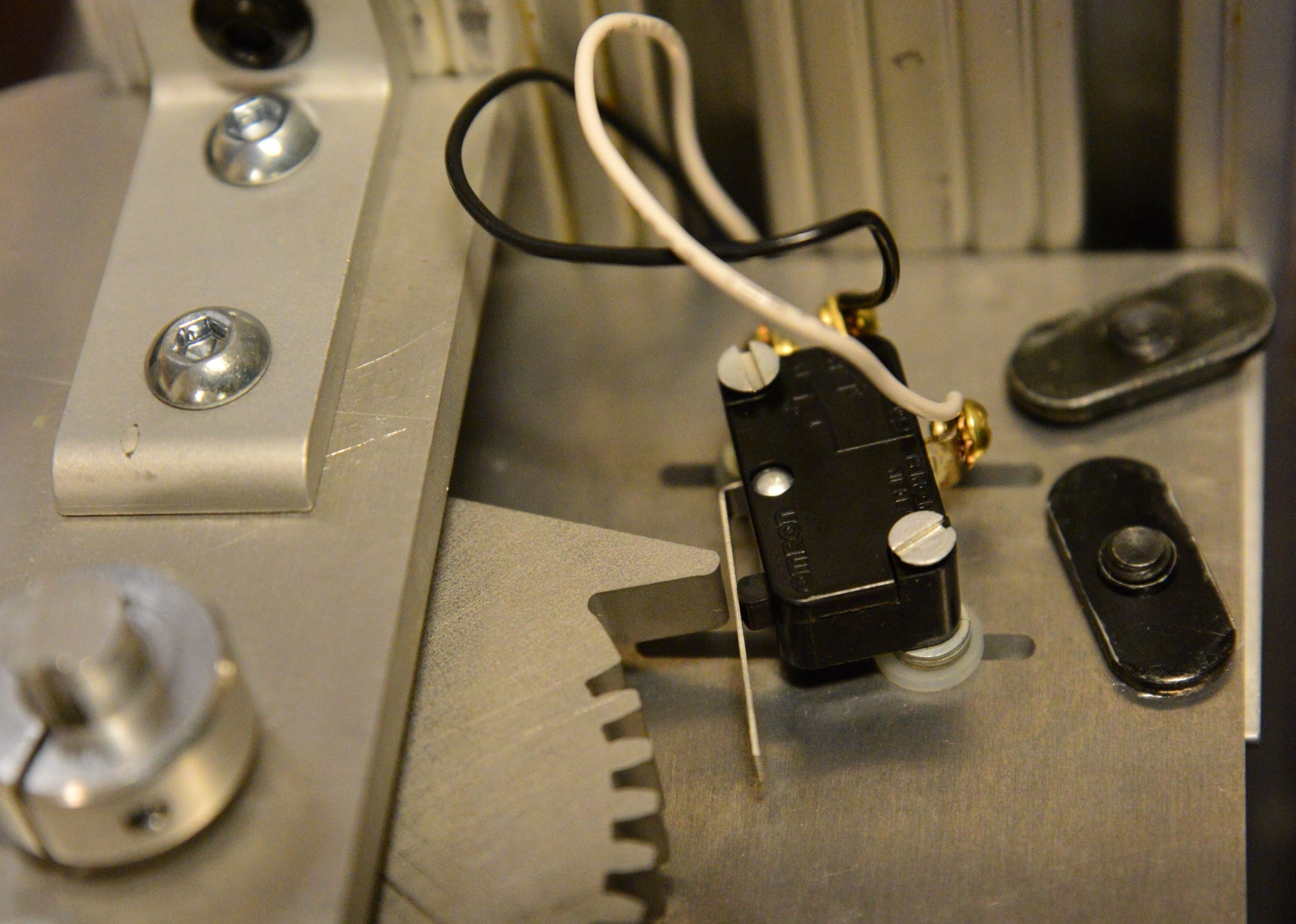
Here is a close-up of the gear-train for actuating the arms. The arms are geared together directly which forces them to move together and apart in sync. The geared motor drives one of the arms. On the right you can see a limit switch that tells the machine when the arms are fully open. This helps the machine locate arm position when it turns on. The switch is mounted on channels so that the position is adjustable.
Note: Other homing and sensing is possible as a function of the position feedback method chosen.
Version 1 – Retired
Insight gathered from the earlier prototype was condensed into a simplified model that is one step closer to a product designed for manufacture. We were able to dial in the dimensions after trial and error with the prototype.
Note the rigid structure and adjustability limited to the bag supports. The fingers that grip the bag should be carefully smoothed to avoid abrasion to the bag. This unit continues to rely on a DC motor. Other motor options are possible.
Download the CAD files here

Caution: Forces and torques are much higher than expected when an Ambu bag is connected to a human respiratory system pressures can range up to 40 cm H2O and, potentially, even higher depending on breath rate. There must be a pressure release valve set at 40 cm H2O; without this higher pressures will risk permeant injury or death. Diseased lungs can have compliance on the order of 10x lower than that of healthy patients and this further compounds the problem. Any testing done without back pressure is invalid.
Early Version
An early prototype unit is shown below in laser cut acrylic. Version 1 was similar and underwent testing. Structural deficiencies were identified, as a result of the red note above, and Version 2 was fabricated with an 80/20 metal frame, to address durability and maximise flexibility during testing.
 MIT E Vent being tested.
MIT E Vent being tested.
 MIT E Vent being tested.
MIT E Vent being tested.
 MIT E Vent being tested.
MIT E Vent being tested.
 MIT E Vent being tested.
MIT E Vent being tested.
 MIT E Vent being tested.
MIT E Vent being tested.
 MIT E Vent being tested.
MIT E Vent being tested.

Recent Comments